Chronic Obstructive Pulmonary Disease (COPD) is one of the leading causes of chronic illness and hospitalization worldwide. Accurate diagnosis and medical coding are essential for ensuring proper patient care, clinical documentation, insurance reimbursement, and regulatory compliance. ICD-10 Code J44.9 is assigned when a healthcare provider diagnoses Chronic Obstructive Pulmonary Disease (COPD) without specifying complications such as an acute lower respiratory infection or acute exacerbation.
For healthcare providers, coders, and medical billers, understanding the correct use of the J44.9 diagnosis code is critical to reducing claim denials, improving coding accuracy, and maintaining compliance with ICD-10-CM coding guidelines. This guide explains the code definition, documentation requirements, coding rules, reimbursement considerations, and best practices.
What Is ICD-10 Code J44.9?
ICD-10 Code J44.9 represents:
J44.9 – Chronic Obstructive Pulmonary Disease, Unspecified
This diagnosis code is part of the ICD-10-CM respiratory disease chapter and is used when the provider documents COPD but does not specify whether the condition includes:
- Acute exacerbation
- Acute lower respiratory infection
- Other specified complications
The COPD ICD-10 code J44.9 is commonly reported in outpatient clinics, physician offices and hospital settings when documentation supports uncomplicated COPD.
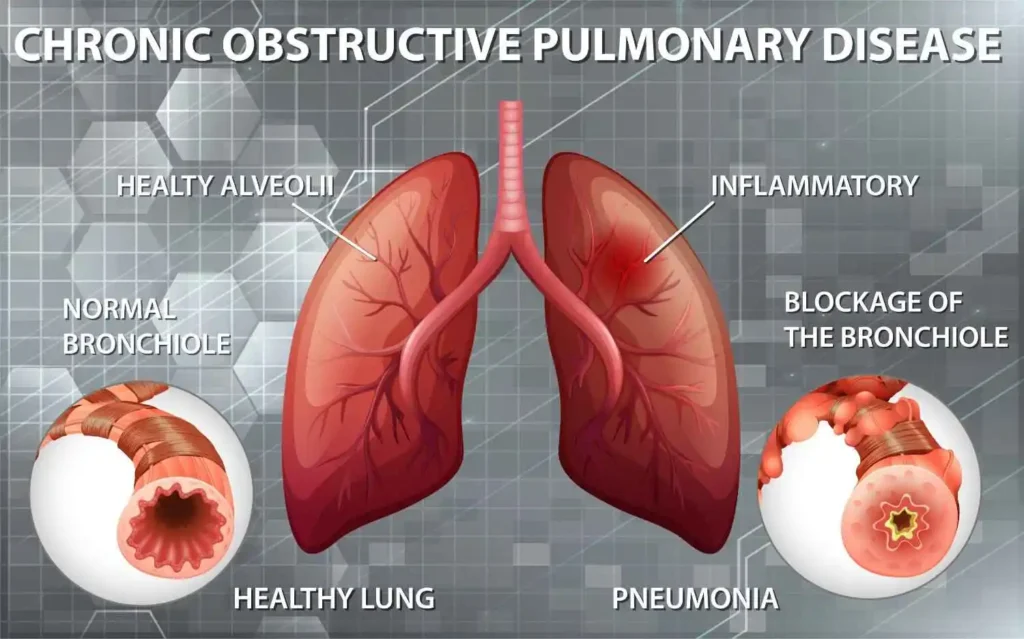
What Is Chronic Obstructive Pulmonary Disease (COPD)?
Chronic Obstructive Pulmonary Disease is a progressive lung disease that restricts airflow and makes breathing difficult. It usually develops over many years and is commonly associated with long-term smoking or exposure to harmful airborne irritants.
Common symptoms include:
- Persistent cough
- Chronic mucus production
- Wheezing
- Shortness of breath
- Chest tightness
- Frequent respiratory infections
- Fatigue
Although COPD cannot be cured, early diagnosis and treatment help slow disease progression and improve quality of life.
When Should ICD-10 Code J44.9 Be Used?
The Chronic obstructive pulmonary disease ICD-10 code J44.9 should be assigned only when provider documentation clearly identifies COPD without mentioning additional complications.
Use J44.9 when documentation states:
- COPD
- Chronic obstructive pulmonary disease
- Stable COPD
- COPD without exacerbation
- COPD unspecified
Do not assign J44.9 if documentation specifies:
- COPD with acute exacerbation
- COPD with acute bronchitis
- COPD with pneumonia
- COPD with lower respiratory infection
These situations require different ICD-10-CM codes.
ICD-10 Coding Guidelines for J44.9
Following official J44.9 coding guidelines helps ensure accurate code assignment.
Important coding principles include:
- Code only conditions documented by the healthcare provider.
- Do not assume exacerbation unless documented.
- Review the complete medical record before assigning a diagnosis code.
- Use the highest level of specificity available.
- Assign additional diagnosis codes when applicable.
Medical coders should always verify documentation before submitting claims.
Documentation Requirements for J44.9
Proper clinical documentation is essential for accurate coding and reimbursement.
J44.9 documentation requirements include:
- Confirmed diagnosis of COPD
- Physician assessment
- Clinical signs and symptoms
- Patient history
- Smoking status when documented
- Diagnostic testing (if available)
- Current treatment plan
- Medication management
Well-documented medical records reduce coding errors and support medical necessity.
Common Diagnostic Tests Used for COPD
Healthcare providers often rely on several diagnostic tools to confirm COPD.
Common tests include:
- Pulmonary function tests (Spirometry)
- Chest X-ray
- CT scan
- Blood oxygen testing
- Arterial blood gas analysis
- Physical examination
- Smoking history evaluation
These tests help determine disease severity and appropriate treatment.
J44.9 Reimbursement Considerations
Accurate coding directly affects insurance reimbursement.
The J44.9 reimbursement process depends on several factors, including:
- Medical necessity
- Complete documentation
- Correct ICD-10 coding
- CPT procedure codes
- Insurance payer policies
- Place of service
Incomplete documentation may lead to:
- Claim denials
- Payment delays
- Medical record audits
- Compliance risks
Accurate coding improves revenue cycle performance while maintaining payer compliance.
COPD Medical Billing Best Practices
Effective COPD medical billing requires collaboration between providers, coders, and billing professionals.
Best practices include:
- Verify diagnosis documentation
- Review coding updates annually
- Confirm medical necessity
- Link diagnosis with performed services
- Monitor payer-specific guidelines
- Conduct routine coding audits
- Educate clinical staff on documentation
These practices improve clean claim rates and reduce reimbursement issues.
Common Coding Errors to Avoid
Medical coders should avoid several common mistakes when reporting COPD diagnosis coding.
Frequent coding errors include:
- Coding exacerbation without provider documentation
- Using unspecified codes when greater specificity exists
- Missing secondary diagnosis codes
- Ignoring physician notes
- Coding suspected conditions as confirmed diagnoses
- Failing to review discharge summaries
Careful documentation review significantly reduces coding inaccuracies.
Difference Between J44.9 and Other COPD ICD-10 Codes
| ICD-10 Code | Description |
|---|---|
| J44.9 | COPD, unspecified |
| J44.0 | COPD with acute lower respiratory infection |
| J44.1 | COPD with acute exacerbation, unspecified |
| J43.- | Emphysema |
| J41-J42 | Chronic bronchitis |
Selecting the correct code depends entirely on provider documentation
Tips for Accurate COPD Diagnosis Coding
Healthcare organizations can improve coding accuracy by following these recommendations:
- Review complete provider documentation
- Verify diagnosis specificity
- Follow Official ICD-10-CM Guidelines
- Stay updated with annual coding revisions
- Communicate with physicians for clarification
- Perform internal coding audits
- Train coding staff regularly
Accurate coding improves patient records while reducing financial risk.
Why Accurate ICD-10 Coding Matters
Correct diagnosis coding benefits everyone involved in patient care.
Benefits include:
- Faster insurance reimbursement
- Reduced claim denials
- Improved compliance
- Better patient data
- Higher coding accuracy
- Reliable healthcare reporting
- Stronger revenue cycle management
Accurate coding also contributes to healthcare quality reporting and public health research.
Frequently Asked Questions (FAQs)
1. What is ICD-10 Code J44.9?
ICD-10 Code J44.9 identifies Chronic Obstructive Pulmonary Disease (COPD), unspecified, when no acute exacerbation or lower respiratory infection is documented.
2. When should J44.9 be used?
It should be reported when the provider diagnoses COPD without documenting additional complications or greater specificity.
3. Can J44.9 be used for COPD with acute exacerbation?
No. COPD with an acute exacerbation should generally be coded with J44.1, provided the documentation supports that diagnosis.
4. What documentation supports J44.9?
Documentation should include a confirmed COPD diagnosis, clinical assessment, treatment plan, symptoms, and any relevant diagnostic findings.
5. Does J44.9 affect reimbursement?
Yes. Accurate documentation and proper coding support medical necessity, reduce claim denials, and help ensure appropriate reimbursement.
6. Why is documentation important for COPD coding?
Complete documentation allows coders to assign the most specific ICD-10-CM code, supports payer requirements, and improves compliance.
Conclusion
ICD-10 Code J44.9 plays an important role in accurately reporting Chronic Obstructive Pulmonary Disease (COPD), unspecified. Proper documentation, adherence to J44.9 coding guidelines, and careful review of the medical record are essential for compliant coding and efficient reimbursement. Healthcare providers, medical coders, and billing professionals should work together to ensure every COPD diagnosis is documented with the highest level of specificity available. Doing so not only improves coding accuracy but also enhances patient care, minimizes claim denials, and supports a stronger revenue cycle management process.